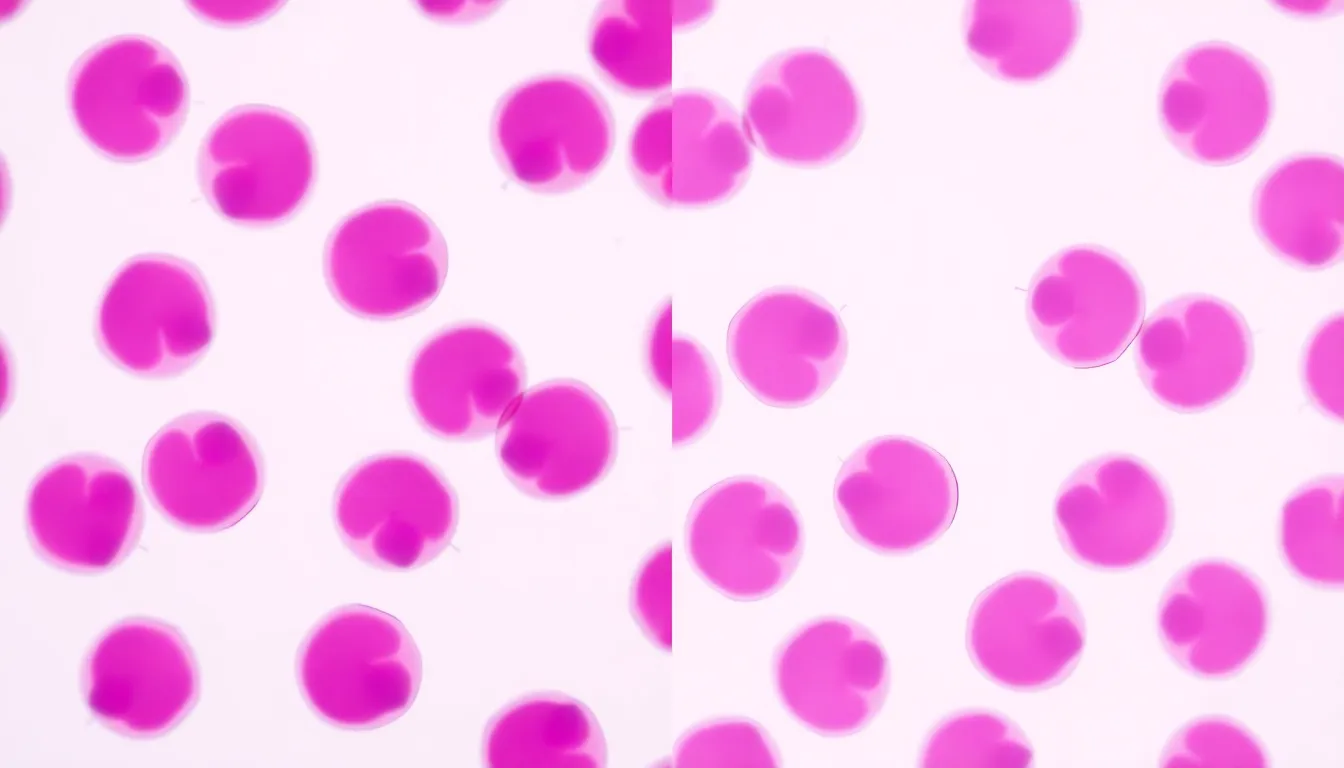
Chronic Lymphoproliferative Disorders (CLPDs) are clonal lymphoid proliferations with indolent behavior.
Sign in to create AI presentations
By signing in, you agree to our Terms of Service and Privacy Policy